Associated Terms:
Hip Laxity, Coxofemoral Laxity, Subluxating Hips, Femoral Head and Neck Excision, Triple Pelvic Osteotomy, Juvenile Pubic Symphysiodesis, Total Hip Replacement, Hip Arthritis
Overview
Canine Hip Dysplasia (CHD) is a condition that begins in dogs as they grow and results in instability or a loose fit (laxity) of the hip joint (Figure 1). The hip joint laxity is responsible for potential clinical signs (symptoms) of hip pain and limb dysfunction and progressive joint changes. The hip joint is a ball and socket joint and continual abnormal movement of the femoral head (ball) deforms the acetabulum (socket). The long-term response to this joint laxity is the progressive loss of cartilage, the development of scar tissue around the joint, and the formation of osteophytes (bone spurs) around the ball and socket (Figure 2).
The cause of CHD is multifactorial; however, hereditary (genetics) is the biggest single risk factor. Rapid weight gain and growth through excessive nutritional intake can complicate the development of CHD. Hip dysplasia occurs most commonly in large breed dogs.
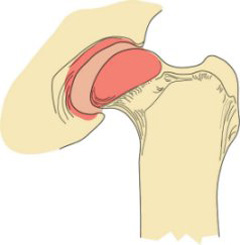
Figure 1. Hip dysplasia presents in dogs as instability of the hip joint. As the dog bears weight, the ball of the femur (thigh bone) moves abnormally relative to the hip socket.
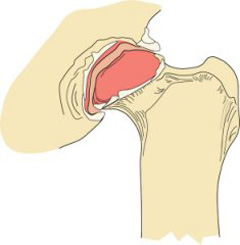
Figure 2. The result of the joint instability is abnormal wear of the cartilage. Cartilage wear leads to the formation of bone spurs and scar tissue, which are the characteristic signs of hip arthritis.
Signs and Symptoms
The symptoms of CHD are lameness (limping), reluctance to rise or jump, shifting of weight to the forelimbs, loss of muscle mass on the rear limbs, and hip pain. Generally, divide dogs with CHD into two groups showing symptoms of CHD:
Group 1: Younger dogs without arthritis, but with significant hip laxity
Group 2: More mature dogs that have developed hip arthritis due to CHD
Dogs may show symptoms at any stage of disease’s development, although many dogs with CHD do not have any obvious symptoms.
Diagnostics

Figure 3. A hip X-ray of a dog with arthritis of the hips as a result of hip dysplasia.
Treatment

Figure 4. A pelvic X-ray of a dog following a TPO. Notice that special plate and screws that hold the pelvis in a rotated position to improve the coverage of the ball by the socket.
Medical treatment entails a combination of multiple modalities to improve your pet’s comfort as much as possible without surgical intervention and includes the use of aggressive weight loss/management, consistent exposure to lower-impact activities (walking, swimming etc.), nonsteroidal anti-inflammatory drugs, physical rehabilitation, fish oil supplements, and disease modifying osteoarthritis drugs. Dogs in Group 1 (see Signs and Symptoms) generally do not respond as well to medical treatment as do dogs in Group 2 (see Signs and Symptoms). For this reason, earlier surgical intervention with procedures such as juvenile pubic symphysiodesis (JPS) or pelvic osteotomy may be indicated.
JPS is a technique for stopping the growth of the pubis (part of the pelvis) to alter the growth/shape of the pelvis, while increasing the ball’s degree of coverage by the socket to diminish hip laxity. It is a relatively minor surgical procedure and puppies less than 18 weeks of age must have it performed. However, since most puppies of this age do not show symptoms of CHD, early diagnosis by way of examination and special X-ray techniques is critical.

Figure 5. A pelvic X-ray of a dog following an FHO. Note the absence of the left femoral head (ball).
Immature dogs with evidence of hip arthritis are not ideal candidates for TPO/DPO, nor are dogs with very severe hip laxity. Dogs need to be screened by examination and X-rays to determine if they may benefit from these procedures. Manage non-candidates medically until they are mature enough for total hip replacement (THR) or femoral head ostectomy (FHO) surgeries.
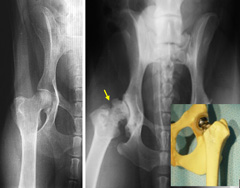
Figure 6. Normal hip (left) and arthritic hip (arrow). Total hip replacement can restore normal structure and function of “ball and socket” joint with implants (color picture).
THR is another option for Group 1 and 2 dogs. This procedure eliminates hip pain and, unlike an FHO, reproduces the mechanics of a normal hip joint producing, more natural range of motion and limb function. As with humans, canine THR involves replacement of both the ball and socket with metal and polyethylene (plastic) implants (Figure 6). These components are fixated in place with bone cement, metal pegs, or “press fit” (bone ingrowth) methods.
Aftercare and Outcome
Risk of complications after JPS are very low; almost all are minor in nature. Success rates for JPS eliminating hip laxity are high and aftercare is very brief, usually just entailing basic incision care and short-term activity restriction.
Reported complications after DPO and TPO include screw loosening, change in limb range of motion, and pelvic canal narrowing. However, the incidence of complications is low and reports of long-term function are expected to be good to excellent.
THR results in an excellent chance of markedly improved limb function. Potential complications after THR include infection, hip dislocation, “loosening” of the implants over time, nerve injury, and femur fracture.
Following both DPO/TPO and THR, the dog’s activity should be restricted to leash exercise outdoors and confinement to a small area indoors until the procedures are deemed healed (via examination and X-rays), generally six and eight weeks respectively. Most pets are weight bearing soon after surgery and require supervision to prevent overuse of the leg during the healing period. If necessary, use a sling for initial assistance with walking. The dog should avoid stairs, slippery surfaces and interactions with other dogs. To get back to normal, slowly increase activity after the initial period of restriction.
Results after FHO vary and are highly dependent upon patient size and proper postoperative physical rehabilitation. While many dogs will have varying degrees of lameness, function should improve when compared with preoperative status. After FHO, pets are encouraged to use the limb as soon as possible in a controlled manner. Aggressive physical rehabilitation and controlled exercise to increase hip range of motion are essential for an optimal outcome. It may take up to six weeks or longer after surgery for some dogs to show improvement.
Content by the American College of Veterinary Surgeons
Leave a Reply